Take, for instance, an embarrassing event from my local hospital. I had a patient with a dorsal foot wound that we had scheduled for a split thickness skin graft.
Scheduled, that is, until two days before, when the OR manager reported
we did not have a dermatome. I was upset to say the least, and embarrassed to tell my patient we had to cancel his surgery. I presented Apligraf as an alternative, which he agreed to with the understanding that his healing would take a little longer. Here's where the interdependence comes in. The OR manager had tried obtaining a loaner
dermatome from three other hospitals in the region with no success. With limited local resources, my hospital relied on others for the instruments, and when they were not available, we looked unprofessional to my patient. The hospital is now obtaining a dermatome.
On the other hand, being a small hospital may be advantageous in that the small size allows for a flexibility not seen with larger institutions. Take my position, for example. I was brought to the area by a cooperative agreement between two rural hospitals who are sharing my expertise. The hospitals share resources in a way that is beneficial to both communities. In large institutions with more complicated administrations, this type of flexibility may be more problematic.
So, as with everything in life, with the good often comes the not-so-good. Best wishes with you and your local hospital.
###
You bring up a good point about showing what we know to the medical community. Recently I got called to the ER dept for a 22 year old male with an acute nail infection. The ER doc was amazed at how fast and adroit I was able to treat this patient, with virtually no pain. When others in the medical community see what we do, more respect will come our way.
—[email protected]
Jarrod,
Your comments about patient compliance are right on target. I particularly like the way you laid out the necessary documentation, patient education and decision making, along with the ultimate role that we must play as the physician. One piece to add is that there is often an appropriate time to FORCE compliance through the application of a total contact cast or by transforming a removable case walker into a non-removable one. This must be reserved for the appropriate patient and wound type, but can have great results.
Your approach and outline of how to handle these patient situations was very well thought out.
—John Steinberg, DPM
PRESENT Editor
Assistant Professor,
Department of Plastic Surgery
Georgetown University School of Medicine
[email protected]
My feeling, after nearly 30 years of practice in both private practice and hospital based settings is that we are occasionally slow to get to the end point. This patient could very easily loose a limb or their life and a straight forward discussion with appropriate W/U and 10 minutes of surgery may well save that limb or life. I used to dance around the difficult discussions, however over the years I have come to realize that patient appreciate a "to the point" sensitive discussion of the most appropriate treatment; you don't have to guarantee anything just that you will do you best to resolve the problem before it becomes a serious issue.
—William Healey, DPM,
FACFAS
Chief,
Foot & Ankle Section
Director,
Podiatric Medical Education
[email protected]
How about considering psychiatric issues. Some patients like to be sick.
—Simon Young DPM
[email protected]
|
###
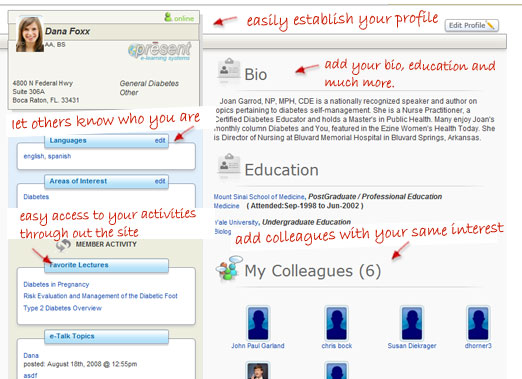
In case you haven't heard, PRESENT Diabetes went live last week with a completely NEW VERSION of its website and it's quite AMAZING. They really have brought Facebook and LinkedIn networking to diabetes care professionals. After you fill out a brief profile, they show you all of the other members with training, interests and experiences similar to your own—and one-click LINKs you to them. You'll have a very useful professional network in no time, and it's not only podiatrists. They already have over 57,000 physician, nursing, dietitian members. Try it by going to https://presentdiabetes.com and make sure you add me to your colleague list!